
How the Willpower Frame Gets It Backwards

The athlete who cannot recover is not failing to push hard enough. The harder they push in that state, the further behind they fall, and that outcome is measurable, not a character judgment. It follows predictably from what happens to the neuroendocrine and autonomic systems under sustained overload without adequate recovery. This is the basic physiology of overtraining syndrome in athletes when training load consistently exceeds the capacity to restore from it.
There is a dominant frame in combat sports training that treats fatigue as a test of will. The athlete who shows up regardless of how they feel is valorized. The athlete who pulls back is seen, and often sees themselves, as soft. This frame is not wrong about the value of discipline, but it is operationally wrong about what the body is doing when it stops responding to training stimulus the way it should.
The central claim of this article is straightforward: what looks like a willpower deficit is, in most cases, a physiological system operating outside its recovery envelope. Effort cannot fix a dysregulated regulatory system. Applied to a system in that state, effort makes the problem worse. This is not a metaphor. It describes specific, measurable changes in the hypothalamic-pituitary-adrenal axis, the autonomic nervous system, the immune system, and the neurochemical systems that regulate motivation and perceived exertion.
Effort cannot fix a dysregulated regulatory system. Applied to a system in that state, effort makes the problem worse.
This article explains what overtraining syndrome is at the biological level, which systems fail and why, and what that means for an athlete managing serious training alongside a demanding career and family. It does not prescribe a training program. It explains the system.
Overreaching Is Not Overtraining: The Spectrum Matters

Overtraining syndrome is the most severe point on a continuum that begins with a normal, productive training response. The spectrum matters because the mechanisms, the timelines for recovery, and the appropriate responses are different at each stage. Collapsing all of them into a single category, being "overtrained," is part of why athletes stay in damaging states longer than they should.
Functional overreaching (FOR) is a deliberate short-term state in which training load exceeds what the athlete can fully recover from in 24 hours. Performance temporarily declines. The key word is temporarily: given adequate recovery following a hard training block, supercompensation occurs and performance exceeds the pre-overreaching baseline. FOR is a planned component of progressive training. It resolves within days to two weeks. (Meeusen et al. 2013)
Non-functional overreaching (NFOR) occurs when training load consistently exceeds recovery capacity without the structured reduction that would allow supercompensation. Performance declines and does not bounce back within a few days of rest. Unlike FOR, NFOR involves early dysregulation of the same hormonal and autonomic systems that, under continued stress, produce full overtraining syndrome. Recovery from NFOR takes weeks to months. (Kreher & Schwartz 2012)
THE THREE STAGES
Functional Overreaching (FOR)
Planned, productive. Performance decline resolves in days to 2 weeks with adequate recovery. Part of progressive training design.
Non-Functional Overreaching (NFOR)
Unplanned sustained overload. Takes weeks to months to resolve. Early dysregulation of hormonal and autonomic systems.
Overtraining Syndrome (OTS)
Pathological state. Requires months of recovery. Diagnosed by exclusion. Different regulatory state from NFOR, not just more severe.
Overtraining syndrome (OTS) is a pathological state requiring months of recovery. It is characterized by measurable neuroendocrine, autonomic, and immune dysregulation, not just performance decline or fatigue. The distinction between NFOR and OTS matters because OTS is not simply more severe NFOR. It represents a different regulatory state with different biological markers and a substantially longer recovery arc.
The diagnostic problem is that OTS has no single biomarker. It is identified by ruling out other causes of sustained performance decline, including illness, nutritional deficiency, psychological stress, and iron-deficiency anemia, combined with the duration and severity of symptoms. (Kreher & Schwartz 2012) This diagnostic complexity is part of why OTS is chronically underidentified: athletes and coaches who cannot see a number on a test are inclined to attribute the problem to something else. The something else is usually effort.
The same cultural pressure that reframes NFOR as a character test is what drives athletes from NFOR into OTS.
The same cultural pressure that reframes NFOR as a character test is what drives athletes from NFOR into OTS. More effort is the mechanism of that progression, not the solution to it.
OTS is not simply more severe NFOR. It represents a different regulatory state with different biological markers and a substantially longer recovery arc.
The HPA Axis: How the Brain's Stress Regulator Breaks Down Under Chronic Load
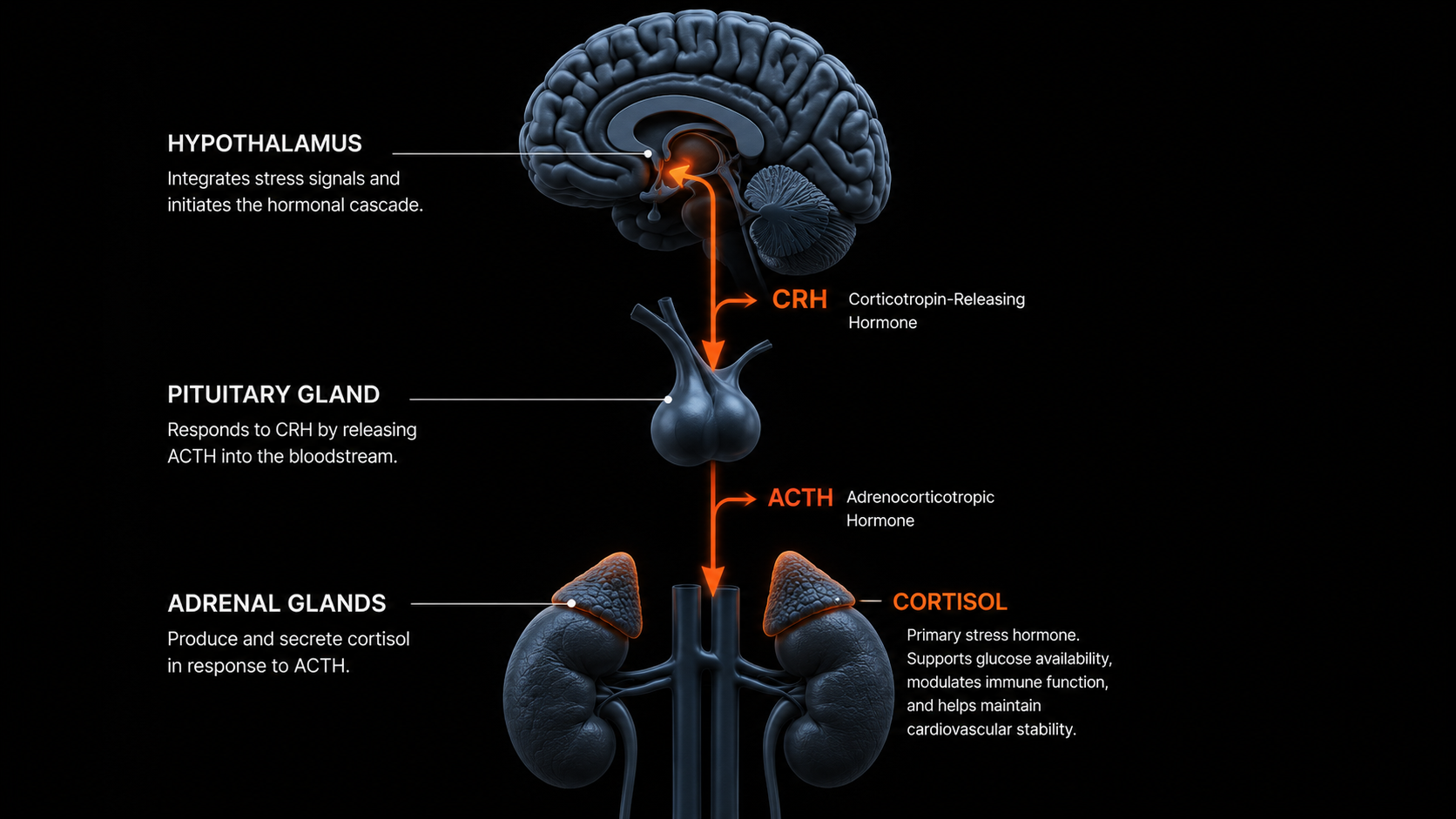
The hypothalamic-pituitary-adrenal axis is the body's primary stress regulation system. The sequence is straightforward: the hypothalamus detects a stressor and releases corticotropin-releasing hormone (CRH), which signals the pituitary to release adrenocorticotropic hormone (ACTH), which signals the adrenal cortex to release cortisol. This cascade handles exercise stress in the same way it handles psychological stress, sleep deprivation, and illness. The axis does not distinguish between stressor types. It integrates them.
Under normal training conditions, this is adaptive. Cortisol mobilizes energy substrates, reduces inflammation acutely, and increases glucose availability and cardiac output in preparation for training demands. The problem arises when the axis is activated repeatedly without the recovery time required to restore baseline function.
Chronic training load without adequate recovery produces two distinct HPA failure patterns depending on training modality and individual response. (Kreher & Schwartz 2012) In one pattern, common in power and strength athletes, the axis remains chronically hyperactive: cortisol stays elevated even at rest. In the other, more common in high-volume endurance athletes, the axis becomes hyporesponsive: it stops producing an adequate cortisol response even when a stressor demands one. Both represent regulatory failure, and both produce measurable performance decline.
SYMPATHETIC OTS
Chronically Elevated Cortisol
Axis remains hyperactive. Cortisol elevated at rest. More common in power and strength athletes.
PARASYMPATHETIC OTS
Blunted Cortisol Response
Axis becomes hyporesponsive. Fails to produce adequate cortisol under stress. More common in high-volume endurance athletes.
The downstream consequences of cortisol dysregulation compound across multiple systems. Chronically elevated cortisol suppresses immune function, impairs glycogen resynthesis in muscle and liver, reduces muscle protein synthesis, and degrades sleep architecture by preventing the normal evening decline in cortisol that allows sleep onset. These are not symptoms of tiredness in the colloquial sense. They are measurable biological changes that make the athlete less capable of responding to training stimulus and less capable of recovering from it.
One compounding factor that is easy to underestimate is the stressor convergence problem. Because the HPA axis does not differentiate between training stress and non-training stress, the athlete who arrives at evening practice after a high-pressure work day and three hours of interrupted sleep is not arriving at baseline. Their axis is already partially activated. The training session lands on a system that has less adaptive capacity than the session is designed to require. The same external training load produces a higher biological cost under those conditions than it would under full recovery.
The axis does not distinguish between stressor types. It integrates them.
The Cortisol/Testosterone Ratio: A Window Into Anabolic State
The cortisol/testosterone ratio provides a concrete way to understand the anabolic-catabolic balance that HPA dysregulation produces. Cortisol is catabolic: it breaks down tissue to mobilize energy. Testosterone is anabolic: it drives tissue synthesis, muscle repair, and adaptation to training stimulus. The ratio reflects which direction the body is currently running. A rising ratio means the body is spending more on stress response than on recovery and growth.
Chronic overloading without adequate recovery raises cortisol and simultaneously suppresses testosterone through its effects on the hypothalamic-pituitary-gonadal axis. The result is a net catabolic state: the athlete is training but not rebuilding at the rate the training requires. This is why overtrained athletes lose strength and lean mass despite continuing to train, and why the intuition that more work will fix declining performance is physiologically backwards. (Urhausen et al. 1995)
Chronically elevated cortisol suppresses immune function, impairs glycogen resynthesis in muscle and liver, reduces muscle protein synthesis, and degrades sleep architecture.
Sleep deprivation compounds the ratio shift independently of training load. Poor sleep elevates morning cortisol and suppresses testosterone, compressing the already-limited recovery window that exists between sessions. Caloric restriction adds a third vector. An athlete managing heavy training load, high work and family stress, inconsistent sleep, and suboptimal nutrition may find the cortisol/testosterone ratio consistently dysregulated even at training volumes that would be fully manageable under better recovery conditions.
The ratio is used clinically as one of several markers for screening NFOR and OTS. It is not diagnostic on its own. No single marker is. Its value is as part of a multi-marker picture that provides earlier detection of regulatory failure than waiting for performance decline to become obvious.
The Autonomic Nervous System Under Chronic Load: And How to Measure What It's Telling You

The autonomic nervous system manages the balance between sympathetic and parasympathetic activity. Sympathetic activity mobilizes resources for effort and stress response: elevated heart rate, reduced digestion, heightened alertness. Parasympathetic activity governs rest, recovery, and repair: lowered heart rate, restored digestive function, tissue regeneration. Healthy training creates a predictable pattern: sympathetic activation during the session, followed by a parasympathetic-dominant recovery window. The extent to which the parasympathetic system can restore baseline between sessions determines effective recovery capacity.
When training load consistently exceeds what the recovery window can restore, the system settles progressively into chronic sympathetic dominance. The parasympathetic recovery window is never fully completed before the next training session activates the sympathetic response again. Over time, the resting state shifts: the stress response remains partially activated, recovery is chronically incomplete, and the physiological cost of each training session accumulates rather than resolving.
The consequences of chronic sympathetic dominance extend across multiple systems simultaneously. Resting heart rate rises because sympathetic tone increases baseline cardiac activation. Sleep degrades because sympathetic activity suppresses slow-wave and REM sleep, with the same cortisol elevation that reflects HPA dysregulation also preventing the evening autonomic shift required for restorative sleep. Stress tolerance decreases because less parasympathetic buffer is available to absorb non-training stressors. Mood becomes less stable. These are not separate symptoms. They are different expressions of the same underlying shift in autonomic balance.
HRV and Resting Heart Rate: Measuring What the ANS Is Doing
Heart rate variability is the most sensitive and accessible non-invasive proxy for parasympathetic activity. It measures the variation in time between consecutive heartbeats. Greater variation reflects stronger parasympathetic tone: the nervous system is actively regulating cardiac intervals, signaling genuine recovery capacity. Lower variation reflects sympathetic dominance: the intervals are more rigid, the parasympathetic influence weaker. (Plews et al. 2013)
HRV is a trend metric, not a single-point reading.
The key insight from the HRV monitoring literature is that HRV is a trend metric, not a single-point reading. One low HRV morning following a hard session or a poor night's sleep is expected and not particularly informative. A sustained downward trend across 7 to 14 days, occurring independent of single hard sessions and persisting into recovery days, is a reliable signal that parasympathetic tone is failing to restore between sessions. That trend typically precedes the onset of obvious subjective fatigue and measurable performance decline by several days, which is what makes it useful as an early-warning signal rather than a lagging indicator. (Plews et al. 2013)
7–14 days
HRV Trend Window for Reliable Overreaching Signal
5–10 bpm
Resting HR Above Baseline: Recognized Overreaching Correlate
Resting heart rate provides a complementary signal measuring the same underlying ANS state from a different angle. Elevated resting heart rate reflects increased sympathetic tone, the same chronic sympathetic dominance that suppresses HRV. Unlike HRV, which requires a wearable with good beat-to-beat accuracy, resting heart rate can be tracked reliably with almost any device. A sustained resting heart rate 5 to 10 beats per minute above an individual's established baseline is a clinically recognized correlate of overreaching and early overtraining. The threshold is not universal, as individual baselines vary, but the directional signal is consistent: rising resting heart rate during a training block indicates that recovery is not keeping pace with load.
Declining HRV paired with rising resting heart rate over the same period is not coincidence or instrumentation noise. Both measures are capturing the same shift in autonomic balance. When both trend together in the wrong direction over multiple days, the signal confidence is substantially higher than either measure alone would provide.
Declining HRV paired with rising resting heart rate over the same period is not coincidence or instrumentation noise.
The Open Window: Why Overtrained Athletes Get Sick More Often

Following a bout of intense or prolonged exercise, there is a transient period during which immune function is measurably suppressed. Several components of the immune system, including mucosal IgA (mucosal immunoglobulin A), natural killer cell activity, and neutrophil function, decline in the hours following heavy exertion. This creates what exercise immunologists have called the open window: a period of reduced host defense during which viral and bacterial pathogens face less immune resistance. (Nieman 1995) The window's duration varies depending on which immune parameter is measured, with estimates ranging from 3 to 72 hours depending on exercise intensity and duration.
3–72 hrs
Duration of Post-Exercise Immune Suppression Window
Under a training program with adequate recovery between sessions, immune function is substantially restored before the next session creates another open window. The windows are transient and do not overlap. In chronic overloading, recovery is insufficient, and consecutive open windows begin to extend into each other. The athlete is not experiencing episodic post-exercise immune suppression. They are experiencing a chronically immunosuppressed state, with baseline immune capacity continuously reduced from what it would be under adequate recovery.
Chronically elevated pro-inflammatory cytokine burden, including IL-6 (interleukin-6) and TNF-alpha (tumor necrosis factor-alpha), contributes to the immune suppression and also to the systemic fatigue, mood disruption, and motivational changes associated with established OTS. (Petersen & Pedersen 2005) These cytokines are not simply markers of overreaching. They feed back into the HPA axis and the central nervous system, compounding the hormonal and neurological dysregulation already in progress.
In chronic overloading, recovery is insufficient, and consecutive open windows begin to extend into each other.
Frequent minor illness during a training block, including upper respiratory tract infections that take longer than usual to resolve and colds that keep returning, is consistent with the elevated infection risk documented in the overreaching literature. (Nieman 1995) It is not bad luck. It is a predictable consequence of immune window stacking and elevated cytokine burden, and an athlete who notices this pattern is observing a genuine physiological signal, not a coincidence of timing.
A second compounding dynamic runs through the illness pattern. Illness forces unplanned rest. After recovering from the illness, the athlete frequently returns to training with higher-than-normal intensity to compensate for lost volume, which restarts and accelerates the cycle of immune suppression that produced the illness in the first place.
These cytokines are not simply markers of overreaching. They feed back into the HPA axis and the central nervous system, compounding the hormonal and neurological dysregulation already in progress.
Central Fatigue: Why the Brain, Not the Muscle, Is the Rate Limiter

Central fatigue and peripheral fatigue are distinct mechanisms that occur simultaneously but through different pathways. Peripheral fatigue is localized to the muscle: substrate depletion, metabolite accumulation, impaired calcium handling at the sarcoplasmic reticulum, and reduced neuromuscular junction efficiency. These are the mechanisms of acute exercise-induced fatigue that the athlete can feel in a specific muscle group. Central fatigue originates upstream, in the brain and spinal cord, and manifests as increased perceived exertion at a given intensity, reduced motor drive, and motivational loss that is independent of the muscle's actual contractile state. Both coexist during exercise, and OTS specifically amplifies the central component. (Kreher & Schwartz 2012)
PERIPHERAL FATIGUE
Origin: Muscle
Substrate depletion, metabolite accumulation, calcium handling impairment, neuromuscular junction efficiency. Felt as localized burn in specific muscle groups. Present in OTS but not the rate limiter.
CENTRAL FATIGUE
Origin: Brain and Spinal Cord
Serotonin/dopamine ratio dysregulation, increased motor drive cost, elevated perceived exertion. Felt as motivational loss, effort aversion, increased RPE. Specifically amplified by OTS — the primary failure mode.
The serotonin hypothesis of central fatigue proposes that during prolonged exercise, increased plasma availability of tryptophan, relative to the branched-chain amino acids that compete with it for transport across the blood-brain barrier, leads to increased serotonin synthesis in the brain. Serotonin is associated with sleep, lethargy, and reduced motivation. Chronically elevated training volume may sustain this elevated serotonin state, contributing to the persistent mood flattening and motivational loss characteristic of OTS. The evidence is suggestive but not definitive: several well-designed pharmacological studies that attempted to manipulate serotonin levels during exercise failed to reliably alter exercise capacity, indicating that serotonin may not be acting as a simple causal switch. (Meeusen et al. 2007)
The current working model involves the serotonin-to-dopamine ratio rather than serotonin alone. Dopamine is central to motivated behavior, effort initiation, and the cognitive experience of reward anticipation. A high serotonin-to-dopamine ratio is associated with fatigue, lethargy, and motivational withdrawal. A low ratio is associated with maintained motivation and arousal. Chronic overloading that sustains elevated serotonin while reducing dopaminergic signaling produces a neurochemical state in which initiating or maintaining training effort is genuinely more costly at the neural level, not just at the perceptual level. (Meeusen et al. 2007)
Chronic overloading that sustains elevated serotonin while reducing dopaminergic signaling produces a neurochemical state in which initiating or maintaining training effort is genuinely more costly at the neural level.
A commonly reported clinical correlate of central fatigue in OTS is increased perceived cost of movement at submaximal loads. Efforts that previously felt manageable begin to feel significantly harder at the same measured intensity. Heart rate, lactate, and power output may be unchanged, but the internal experience of the effort has shifted upward — this is the same mechanism described in central governor theory. This is not deconditioning. It is the central nervous system increasing the perceived cost of movement as a regulatory response to the accumulated neurochemical and hormonal dysregulation already described.
This is where the willpower frame collapses completely. The athlete who cannot make themselves train at normal intensity, who finds sessions they previously looked forward to feeling aversive, who is flat and disengaged in the gym, is experiencing a measurable disruption in the neurochemical systems that generate motivated behavior. What reads as no motivation to workout is not a character deficit. Telling that athlete to want it more is physiologically incoherent. Removing the stressor that is depleting the system is the relevant intervention.
Telling that athlete to want it more is physiologically incoherent.
When Sleep Degrades During a Training Block: What the Body Is Telling You

Sleep disruption during a heavy training block is not incidental. The same cortisol dysregulation and sympathetic dominance described above directly interfere with the neurophysiology of sleep onset and sleep architecture. Cortisol follows a cortisol circadian rhythm, normally peaking in the early morning and declining through the afternoon and evening to allow sleep onset. In states of HPA hyperactivation, whether from training overload, psychological stress, or their combination, this decline is blunted. Elevated evening cortisol acts as a physiological arousal signal at exactly the moment when the system needs to shift into parasympathetic-dominant state for restorative sleep. (Kreher & Schwartz 2012)
What athletes notice during these periods is characteristic: difficulty falling asleep despite physical exhaustion, waking in the early morning hours and being unable to return to sleep, normal sleep duration that produces unrefreshing sleep, and a general sense that rest is not actually restoring them. These are not signs of insomnia in the clinical sense. They are signs that the HPA axis and autonomic nervous system are not allowing the shift into parasympathetic-dominant state that restorative sleep architecture requires.
Poor sleep during overtraining does not simply fail to help. It actively accelerates the regulatory failure already underway.
The compounding structure is important here. Poor sleep quality further elevates morning cortisol independently of training load. It suppresses testosterone through sleep-dependent hormonal processes. It reduces the immune competence already compromised by the open window mechanism, and it delays the neurological recovery that central fatigue requires. Poor sleep during overtraining does not simply fail to help. It actively accelerates the regulatory failure already underway. The athlete who responds to feeling unrecovered by training harder, believing that enough effort will eventually fix the sleep problem, is running the wrong causal model.
Tracking Overtraining Markers: What the Numbers Actually Tell You
No single marker reliably identifies OTS, NFOR, or even meaningful overreaching. Any single reading in isolation is noise. The signal is in sustained trends across multiple markers, observed over a period long enough to distinguish a response to a hard training week from a deteriorating regulatory trajectory. Athletes who track one metric and act on individual readings are using a weak tool poorly, which is not an argument against tracking, but an argument for understanding what tracking can and cannot tell you. (Urhausen & Kindermann 2002)
The accessible marker cluster that provides meaningful signal without requiring blood draws consists of HRV trend, resting heart rate trend, sleep quality self-report, mood and motivation self-report, and performance output at fixed intensity with tracked perceived exertion. A sustained pattern of degradation across three or more of these markers over 7 to 14 days is a more reliable signal than any single measurement. The multi-marker picture provides the context that individual readings cannot.
THE 5-MARKER CLUSTER
HRV Trend
Sustained decline over 7–14 days (not single readings) signals parasympathetic failure to restore between sessions.
Resting Heart Rate Trend
Rising trend 5–10 bpm above personal baseline signals chronic sympathetic dominance.
Sleep Quality
Self-reported. Degraded quality across multiple nights, unrefreshing despite adequate duration.
Mood and Motivation
Persistent loss of drive across multiple days. Not one bad day.
Perceived Exertion at Fixed Intensity
Increasing RPE at measurable constant outputs across sessions — not explained by intensity or volume changes.
The signal is in sustained trends across multiple markers, observed over a period long enough to distinguish a response to a hard training week from a deteriorating regulatory trajectory.
What the marker cluster can confirm is that ANS and CNS dysregulation are present and are not resolving with normal rest. What it cannot establish is whether the state is FOR, NFOR, or OTS. That distinction depends primarily on recovery duration. FOR resolves within two weeks of adequate reduced load. NFOR takes weeks to months. OTS takes months. If degraded markers have not normalized after two full weeks of substantially reduced training load, NFOR or OTS is the more likely explanation than simple accumulated fatigue.
The measurement lag point is worth internalizing: by the time subjective fatigue is obvious, performance is declining, and motivation is low, the regulatory dysregulation has typically been developing for days to weeks. Tracking provides earlier detection. Not tracking means the athlete is always responding to a problem that has been compounding while they were unaware of it.
Overtraining in BJJ Athletes: Why Combat Sports Training Creates Specific Risk

The overtraining syndrome risk profile for combat sports athletes is structurally different from single-modality sports, and that difference matters for load management. A BJJ, boxing, or Muay Thai training session is not a single physiological stressor. It combines technical drilling, which carries its own cognitive and motor learning load; live sparring, which adds both physical intensity and competitive psychological activation; and in many gyms, supplementary conditioning work. The CNS and HPA load cannot parse these stressors separately. They integrate them. A two-hour BJJ session may produce an HPA and ANS load that is not captured in simple volume or heart rate metrics.
The hobbyist athlete training around a full career and family faces a compounding problem. They arrive at practice with a cortisol load that reflects not only their previous training sessions but their entire day: work deadlines, difficult decisions, family obligations, traffic, and inadequate sleep the night before. These are real HPA inputs. The person who trains four hours per week but manages high background load across the other 164 hours is not training with a low systemic load. They are training with a high background load against which training stress is added. Standard calculations of weekly training volume ignore this entirely.
THREE HIDDEN LOAD FACTORS
Technical Drilling
Motor learning and cognitive processing create CNS load that doesn't appear in heart rate or volume metrics.
Live Sparring
Adds competitive psychological activation (HPA input) on top of physical intensity — stressors sum, not average.
Background Stressor Load
Work, family, and sleep deficits across the other 164 hours per week are real HPA inputs that compound training stress.
Combat sports culture also applies particular pressure at exactly the wrong moments. The valorization of showing up regardless of how you feel, of not tapping, of training through discomfort, is an appropriate norm for the specific demands of skill development under fatigue. It becomes physiologically harmful when applied without distinction to the signals that the autonomic and neuroendocrine systems produce when they are in genuine regulatory failure. The athlete who has been trained to interpret every impulse to pull back as a mental weakness will be slow to recognize NFOR and slower still to recognize OTS. The cultural frame delays the correct response.
The person who trains four hours per week but manages high psychological stress across the other 164 hours is not training with a low systemic load.
The 48-to-72-hour window between sessions in a typical hobbyist training schedule is not automatically sufficient for recovery. Whether it is restorative depends entirely on sleep quality, nutrition, and the total non-training stressor load during that window. Assuming the gap is enough rest is a fixed-input assumption applied to a highly variable system, and it is precisely the assumption that produces NFOR in athletes who appear, by training volume alone, to be managing their load reasonably.
Assuming the gap is enough rest is a fixed-input assumption applied to a highly variable system.
The Mistakes That Drive Athletes From Overreaching Into Overtraining

1
Treating Recovery as Fixed
Training load managed as the only variable; recovery capacity treated as constant. It is not.
2
Applying Yesterday's Baseline
Same external load lands differently on a degraded recovery system than a recovered one.
3
Reading Motivation as Psychology
Motivational loss from dopaminergic disruption is a physiological output, not a character deficit.
4
Under-Estimating Recovery Duration
FOR resolves in days. NFOR takes weeks to months. OTS takes months. "A few days off" is calibrated to the wrong state.
5
Conflating Fitness With Resilience
High training capacity scales the recovery demand. It does not eliminate it.
The most consequential mistake in load management is treating training load as the only variable in the performance equation while treating recovery capacity as fixed. It is not fixed. Recovery capacity is determined by sleep quality, nutritional status, non-training psychological stress, illness history, and the cumulative load of recent training weeks. An athlete managing their training load without monitoring the recovery inputs is optimizing one side of the equation while leaving the other uncontrolled. Understanding how fitness and fatigue accumulate and dissipate at different rates is the foundation of managing this equation correctly.
A second, related mistake is applying yesterday's baseline to today's tolerance. Training tolerance is not static across weeks. An athlete who managed a 90-minute hard sparring session without issue three weeks ago cannot necessarily manage the same session today if sleep has been poor, stress has been high, and the recent training block has been dense. Applying the same external load to a degraded recovery system produces a higher physiological cost than the same load applied to a recovered system. The session looks identical on paper. The biological response is not.
Applying the same external load to a degraded recovery system produces a higher physiological cost than the same load applied to a recovered system.
The third mistake is interpreting motivational loss as a psychological problem and responding by trying to override it with willpower. The dopaminergic and serotonergic disruption described in the central fatigue section is a physiological output of the regulatory failure in progress. Reduced drive to train is not an independent cause of underperformance. It is a consequence of the same mechanism that is producing every other overtraining symptom. Increasing effort in response to motivational loss caused by central neurotransmitter dysregulation is applying more of the stimulus that created the problem.
A fourth mistake, particularly common in NFOR, is treating "a few days off" as sufficient recovery when the timeline does not fit. FOR resolves in days to two weeks. NFOR does not. An athlete who takes a four-day rest period after noticing that something is wrong, returns to training feeling marginally better, then immediately resumes previous load, has not given the regulatory systems the time required to restore baseline function. The four-day window is calibrated to FOR. It is insufficient for NFOR, and dramatically insufficient for OTS. The intuition that a long weekend should fix persistent fatigue is not calibrated to the biological reality of the more severe states.
A fifth mistake deserves attention because it is counterintuitive: confusing high fitness with protected recovery capacity. A highly trained athlete can generate substantially more training load per session than a less-trained athlete, which means the recovery demand from their sessions scales with their fitness, not inversely to it. The assumption that being very fit means the body can handle more without negative consequences conflates performance capacity with recovery resilience. They are related but not the same. High training capacity does not protect against overtraining syndrome; it may increase the risk when load management does not keep pace with adaptation.
High training capacity does not protect against overtraining syndrome; it may increase the risk when load management does not keep pace with adaptation.
Applying the Mechanism: How Understanding This Changes What You Do

The standard load management question is: how much can I train this week? The question that follows from the mechanism described in this article is more productive: what is my current recovery capacity, and what load can that capacity actually absorb? These are not the same question. The first is answered by looking at the training plan. The second requires monitoring the marker cluster, including HRV trend, resting heart rate, sleep quality, mood, and perceived exertion, and interpreting it against the recovery conditions of the preceding week.
THE STANDARD QUESTION
"How much can I train this week?"
Answered by looking at the training plan. Input: volume and intensity only. Recovery capacity assumed fixed.
THE ACCURATE QUESTION
"What load can my current recovery capacity absorb?"
Answered by monitoring the marker cluster: HRV, resting HR, sleep, mood, RPE trends. Recovery capacity treated as a variable.
Treating recovery load as an active variable rather than a passive background condition changes what the athlete pays attention to. Sleep is not ancillary to training. It is a direct input into HPA axis restoration and ANS parasympathetic recovery. Nutritional status, particularly caloric availability and carbohydrate adequacy, affects cortisol levels and glycogen resynthesis independently of training volume. Psychological stress from work and family is not a separate domain from athletic recovery. It shares the HPA axis with training stress. Managing these variables is part of training load management, even when none of the adjustment involves changing what happens inside the gym.
Treating recovery load as an active variable rather than a passive background condition changes what the athlete pays attention to.
Using the marker cluster to detect ANS drift early gives the athlete a tool for responding to regulatory failure before it compounds. A single low-HRV morning or one poor night's sleep does not warrant changing the training plan. A 7-to-14-day trend of declining HRV, rising resting heart rate, degraded sleep quality, and increasing RPE at previously manageable intensities is a signal worth acting on. Reducing load in response to that signal is not giving up on a training block. It is applying the correct response to the condition the system is reporting. Understanding why daily readiness varies gives the marker cluster more interpretive context.
Volume increases warrant particular caution given the measurement lag discussed earlier. The physiological cost of exceeding recovery capacity does not appear immediately in performance metrics. The regulatory systems continue producing adequate outputs for some period while the adaptive ceiling is being exceeded. Conservative volume increases, whether measured by session count, intensity, or duration, give the monitoring system time to detect the regulatory response before it compounds into NFOR. The cost of a conservative increase that turns out to be unnecessary is several weeks of slightly slower volume accumulation. The cost of an aggressive increase that crosses into NFOR is several months of diminished training capacity.
The cost of an aggressive increase that crosses into NFOR is several months of diminished training capacity.
For combat sports athletes specifically, this means accounting for the CNS and psychological load of high-intensity sparring in ways that simple volume metrics do not capture. A week that appears light by session count may carry a high regulatory load if the sessions involved competitive sparring, tournament preparation, or technically demanding drilling under fatigue. The marker cluster matters more for this population, not less. The training variable is noisier, which makes the biological monitoring signal more important as a counterweight.
Frequently Asked Questions
What is the difference between overreaching and overtraining?
Overreaching is a short-term state of elevated training load that exceeds daily recovery capacity. Functional overreaching is planned and resolves within days to two weeks, producing a performance rebound. Non-functional overreaching involves sustained load beyond recovery capacity and takes weeks to months to resolve. Overtraining syndrome is a pathological extension of non-functional overreaching requiring months of recovery, characterized by measurable neuroendocrine, immune, and autonomic system dysregulation. The fitness-fatigue model provides the structural framework for understanding why these states emerge from the asymmetric rates of fitness gain and fatigue accumulation.
How do you know if you are overtrained or just tired?
Normal fatigue resolves within 24 to 48 hours of reduced load. Overreaching and overtraining syndrome do not. The key signals are sustained trends: HRV declining over 7 to 14 days, resting heart rate elevated above individual baseline, sleep quality degrading, motivation dropping, and perceived exertion increasing at fixed intensities. If degraded markers persist beyond two weeks of substantially reduced load, non-functional overreaching or overtraining syndrome is the more likely explanation.
What does low HRV mean for training?
A single low HRV reading is noise, not signal. It reflects the acute response to a hard session or poor sleep. A sustained downward trend in HRV over 7 to 14 days, occurring even on recovery days, indicates that parasympathetic tone is failing to restore between sessions. This is an early sign of autonomic nervous system dysregulation associated with overreaching. HRV should be read as a trend metric, not a day-by-day pass or fail threshold.
Why do overtrained athletes get sick more often?
Intense exercise creates a transient window of immune suppression lasting 3 to 72 hours, during which infection risk increases. Under adequate recovery, immune function restores before the next session. Under chronic overloading, consecutive immune suppression windows overlap, producing a state of chronic reduced immune competence. Elevated inflammatory cytokines associated with sustained overloading further impair immune function and contribute to the systemic fatigue and mood disruption of overtraining syndrome.
How long does it take to recover from overtraining syndrome?
Recovery duration depends on severity. Functional overreaching resolves in days to two weeks with adequate rest. Non-functional overreaching requires weeks to months of substantially reduced load. Full overtraining syndrome requires months. There is no shortcut: the HPA axis, autonomic nervous system, and immune system require time to restore regulatory baseline. Returning to full training volume before markers normalize typically restarts the cycle rather than advancing recovery.
The Bottom Line
Overtraining syndrome in athletes is a regulatory failure, not a motivational one. The HPA axis dysregulates, the autonomic nervous system loses its recovery gradient, the immune system's open window becomes chronic rather than transient, and the neurochemical systems that generate motivated behavior are disrupted by the same accumulated load that produced every other symptom. These are measurable changes in specific biological systems. They respond to removing the stressor, not to adding more of it.
The willpower frame is not simply inaccurate. It is harmful in proportion to how completely an athlete has internalized it, because it directs more effort at a system that cannot absorb more effort. The appropriate response to NFOR or OTS signals is load reduction and recovery management, applied for long enough that the regulatory systems can actually restore baseline function.
Recovery capacity is a variable, not a constant. It fluctuates with sleep, stress, nutrition, and the cumulative load of preceding weeks.
The insight that changes how a serious athlete manages training is not dramatic: recovery capacity is a variable, not a constant. It fluctuates with sleep, stress, nutrition, and the cumulative load of preceding weeks. The athlete who monitors that variable, who treats it as worth tracking the same way they track session volume or performance output, is operating with accurate models produce better outcomes over the long time horizon that competitive longevity requires.
Recovery capacity is not fixed — it is a variable you can track, and the system will tell you when it's failing. More effort into a failing regulatory system does not fix it. It accelerates the breakdown.
The athlete who monitors recovery capacity the same way they monitor training volume is operating with a more accurate model of how adaptation actually works. Over a long training career, that accuracy compounds.
Mydos Performance
— Sustained vs. Borrowed Energy Series —
Overtraining Syndrome in Athletes: Why It's a System Failure, Not a Willpower Problem
The physiology of pushing too hard when the system needs less
By Ricardo Londono · 2026