
Does Caffeine Give You Energy?
Caffeine is the most widely used psychoactive substance in the world, and nearly everyone who asks does caffeine give you energy gets the same answer: it does. That description is wrong. Not imprecise, not incomplete: it is mechanistically incorrect. Caffeine does not generate energy in any physiological sense of the term.
What it does instead is suppress the signal that tells you your energy is depleted. Those are not the same thing, and the difference matters more than most people who rely on caffeine have stopped to consider. A substance that generates energy and a substance that makes you believe you are not tired produce identical short-term feelings. But the cost underneath those identical feelings is very different. If you're always tired despite doing everything right, the signal-suppression mechanism described here is likely part of why.
RESOLVES DEPLETION
Generates Energy
Increases ATP production, oxygen delivery, or substrate availability. The underlying physiological state improves.
MASKS DEPLETION
Hides the Signal
Blocks the receptor that reports depletion. The underlying state is unchanged — only the perception of it is suppressed.
This article explains the mechanism behind both effects: what caffeine actually does at the level of receptor pharmacology, what happens when that pharmacological action ends, and what the cumulative cost of habitual use looks like for a person who trains seriously under sustained load. The goal is not to argue that caffeine is harmful - the benefits are actually very well-established. The goal is to give you enough mechanistic clarity to evaluate whether your current caffeine use is producing net benefit or net debt.
What it does instead is suppress the signal that tells you your energy is depleted.
Borrowed Energy vs. Resolved Energy

Before the receptor pharmacology, a conceptual distinction is worth establishing, because it frames everything that follows. Two categories of intervention affect what we experience as energy and alertness. The first category includes interventions that increase the actual availability of metabolic resources: more ATP production, better oxygen delivery, improved substrate availability. These resolve the underlying physiological state. The second category includes interventions that reduce the perception of depletion without changing that underlying state. They mask the signal rather than address the source.
ENERGY INTERVENTION TYPES
RESOLVES DEPLETION
Increases actual metabolic resource availability (ATP production, oxygen delivery, substrate). Underlying physiological state improves. Recovery cost is proportional to work done.
MASKS DEPLETION
Reduces the perception of depletion without changing the underlying state. Underlying deficit accumulates. Recovery cost is deferred, not eliminated.
Caffeine belongs entirely in the second category. It produces no ATP. It does not increase oxygen-carrying capacity or accelerate glycolytic or oxidative metabolism in any meaningful way. The energy you feel after consuming caffeine was not created by the caffeine; it was already there, unperceived because the perception system was suppressed.
The practical consequence of this distinction is straightforward: interventions that resolve fatigue allow harder training at roughly equivalent recovery cost. Interventions that mask fatigue allow harder training at higher recovery cost, because the underlying depletion continues accumulating while the perception of it is blocked. This is what borrowed energy means at the mechanism level. The debt is not a metaphor. It accrues in the same physiological systems caffeine temporarily hides. The fitness-fatigue model provides the structural framework for understanding why this deferred cost eventually surfaces as declining net performance.
Interventions that mask fatigue allow harder training at higher recovery cost, because the underlying depletion continues accumulating while the perception of it is blocked.
What Adenosine Is and Why It Accumulates

Adenosine is a purine nucleoside. Every time a cell hydrolyzes ATP to release energy, adenosine is produced as a downstream metabolite. Under normal metabolic conditions, adenosine is continuously generated and continuously cleared, but during periods of high neuronal activity or sustained energy expenditure, production outpaces clearance and extracellular adenosine concentrations rise.
In the brain, adenosine functions as a neuromodulator. As it accumulates in the extracellular space, it binds to inhibitory adenosine receptors and progressively reduces neuronal excitability. This is the biological mechanism behind the increasing sense of heaviness and fatigue and reduced drive that builds over a long day or a hard training session. Research establishing that adenosine accumulates during prolonged wakefulness and declines during recovery sleep identified it as a key mediator of what sleep scientists call homeostatic sleep pressure (Porkka-Heiskanen et al. 1997). The link between adenosine and energy metabolism, specifically the finding that neuronal activity both consumes energy and raises extracellular adenosine concentrations, has been reviewed extensively (Porkka-Heiskanen et al. 2011).
WAKEFULNESS PATHWAY
Hours Awake → Adenosine Rises
Slow homeostatic buildup. The longer you have been awake, the higher the adenosine load. This is the normal sleep-pressure mechanism.
EXERCISE PATHWAY
Metabolic Intensity → Adenosine Spikes
Faster, localized accumulation during high-intensity activity. Adenosine tracks how hard you have been working, not just how long you have been awake.
Adenosine accumulation follows two distinct patterns relevant to athletes. The first is slow homeostatic buildup during wakefulness: the longer you have been awake, the higher your adenosine load. The second is faster, more localized accumulation during metabolically intense activity. Research in rodent models suggests that high-intensity exercise elevates brain adenosine concentrations significantly, while moderate exercise does not produce the same effect (Elbin 2007) . This means adenosine tracks both how long you have been awake and how hard you have been working, making it a dual readout of metabolic expenditure relevant to any serious athlete.
Adenosine is not a waste product in any pejorative sense. It is an accurate physiological signal of metabolic demand. The fatigue and reduced drive it produces are informational. That context matters for what comes next, because caffeine does not address that information; it suppresses the messenger.
Adenosine is not a waste product in any pejorative sense. It is an accurate physiological signal of metabolic demand.
How Caffeine Blocks Adenosine Receptors

Caffeine's primary mechanism of action is competitive antagonism at adenosine receptors, principally the A1 and A2A subtypes (Fredholm et al. 1999). A1 receptors are widely distributed throughout the brain and modulate neuronal excitability broadly; A2A receptors are concentrated in regions associated with arousal, attention, and motor control. At the concentrations achieved from typical human caffeine intake (the equivalent of one to three cups of coffee), caffeine occupies these receptor binding sites without activating them.
Competitive antagonism means caffeine and adenosine compete for the same binding sites. While caffeine is bound, adenosine cannot bind, and the fatigue signal is not transmitted. This is why caffeine produces its characteristic effects on alertness and perceived effort. It is not generating a new alertness signal; it is blocking the signal that would reduce alertness.
WHAT COMPETITIVE ANTAGONISM DOES NOT DO — 01
Does Not Degrade Adenosine
Caffeine has no effect on the adenosine molecule itself. It continues to accumulate at the same rate throughout the blockade period.
WHAT COMPETITIVE ANTAGONISM DOES NOT DO — 02
Does Not Accelerate Clearance
The rate at which adenosine is removed from the extracellular space is unchanged. Clearance mechanisms operate identically with or without caffeine present.
WHAT COMPETITIVE ANTAGONISM DOES NOT DO — 03
Does Not Reduce Synthesis
Adenosine production from ATP hydrolysis continues uninterrupted. Every cellular energy transaction still generates adenosine as a byproduct.
The critical mechanistic detail, and the one most often missed in popular accounts of caffeine, is what competitive antagonism does not do. Caffeine does not degrade adenosine. It does not accelerate adenosine clearance. It does not reduce adenosine synthesis. Throughout the entire period that caffeine occupies adenosine receptors, adenosine continues to accumulate in the extracellular space at the same rate it would without caffeine. The molecule is present and building. Only the receptor is blocked.
It is also worth noting that caffeine's downstream effects on dopamine and norepinephrine systems are real but secondary. They are a consequence of adenosine blockade releasing inhibition on other neurotransmitter pathways, not a primary mechanism. Framing caffeine primarily as a dopamine drug, as some popular neuroscience coverage does, misrepresents the pharmacology.
Throughout the entire period that caffeine occupies adenosine receptors, adenosine continues to accumulate in the extracellular space at the same rate it would without caffeine.
The molecule is present and building. Only the receptor is blocked.
The Caffeine Crash: Why It Happens

Caffeine is metabolized primarily in the liver by the CYP1A2 enzyme system. Its half-life in most healthy adults averages approximately five to six hours, though substantial individual variation exists. A systematic analysis of caffeine pharmacokinetic data from 141 publications documented a range from approximately 2.3 to 9.9 hours, driven by genetic variation in CYP1A2 activity, smoking status, use of oral contraceptives, age, and liver function (Grzegorzewski et al. 2022). What this means practically: a dose consumed at 6 PM can still be pharmacologically active at midnight for a significant portion of the population.
2.3 hrs
MINIMUM HALF-LIFE
5–6 hrs
AVERAGE HALF-LIFE
9.9 hrs
MAXIMUM HALF-LIFE
Source: Grzegorzewski et al. 2022 (Frontiers in Pharmacology)
As caffeine is metabolized and its concentration falls, receptor occupancy declines. The adenosine that accumulated during the blockade period, unrestrained and uncleared, continuing to build throughout the time caffeine held the receptor, is now free to bind simultaneously. The result is a rapid shift from suppressed fatigue perception to elevated fatigue perception. This is the crash.
The Debt Builds While It Is Hidden
Illustrative. While caffeine holds the receptor, fatigue is hidden — when it clears, the accumulated signal arrives at once.
The crash is not caused by caffeine wearing off. It is caused by adenosine that was prevented from signaling earlier signaling all at once. The debt was accruing the entire time; what changes when caffeine clears is not the debt itself but the sudden visibility of it. The magnitude of the rebound correlates predictably with dose, duration of blockade, and the pre-existing adenosine load at the time caffeine was consumed. A higher dose blocks more receptors for longer; a higher baseline adenosine load means more adenosine is available for simultaneous binding when blockade ends. Both factors produce a steeper crash.
This is the acute cost structure of caffeine. The chronic cost structure, what happens to the system over weeks and months of habitual use, is a separate and compounding problem.
The crash is not caused by caffeine wearing off. It is caused by adenosine that was prevented from signaling earlier signaling all at once.
Caffeine Tolerance: What It Actually Means

With repeated caffeine use, the brain adapts. Evidence from human platelet studies suggests that chronic caffeine intake produces upregulation of adenosine receptors: more binding sites are created as a compensatory response to persistent receptor blockade (Daly et.al., 2015). The evidence for upregulation is real but heterogeneous: different studies show different magnitudes across different brain regions, and the mechanism in humans is less directly characterized than in animal models.
Chronic Blockade → More Receptors
THE THREE-STAGE TOLERANCE MECHANISM — 01
Receptor Upregulation
Chronic blockade triggers compensatory production of more adenosine receptor binding sites. The brain increases receptor density in response to persistent antagonism.
THE THREE-STAGE TOLERANCE MECHANISM — 02
Dose Escalation Pressure
More binding sites means the same dose achieves less complete blockade, driving habitual users toward higher doses to maintain the same perceived effect.
THE THREE-STAGE TOLERANCE MECHANISM — 03
Degraded Baseline
With more receptors available when caffeine is absent, adenosine produces a stronger inhibitory effect than it did before habituation began. Baseline alertness falls below pre-habituation levels.
What upregulation means functionally is that more caffeine is required to achieve the same degree of receptor blockade. More binding sites means more competition, which means the same dose of caffeine produces less complete blockade than it did before tolerance developed. This is why habitual users report that caffeine becomes progressively less effective and require increasing doses to achieve the same perceived effect.
Upregulation also changes the baseline state in a more significant way. When caffeine is absent and more receptors are available for adenosine to bind, adenosine produces a stronger inhibitory effect than it would in a non-habituated brain. The baseline alertness of a regular, heavy caffeine user, in the absence of caffeine, is lower than it was before habitual use began. Caffeine does not return them to the alertness they would have as a non-user; it returns them to the alertness they had before habitual use changed their receptor landscape.
The timeline of tolerance development is relevant here. Ergogenic effects appear to diminish relatively rapidly with daily use at performance-relevant doses, and the process is substantially complete within one to two weeks of daily consumption. Tolerance is not a slow drift; it is a relatively rapid pharmacological adaptation.
The baseline alertness of a regular, heavy caffeine user, in the absence of caffeine, is lower than it was before habitual use began.
The Dependency Loop: When Caffeine Recovers What Caffeine Removed

The tolerance mechanism sets up a dependency loop that reframes the question of what caffeine is actually doing for habitual users. The sequence runs as follows: habitual use upregulates adenosine receptors, which lowers baseline alertness in the absence of caffeine, which means caffeine is now required to restore the baseline that previously existed without it. The alertness caffeine provides is, in large part, the recovery of alertness that caffeine-induced adaptation removed.
A Self-Reinforcing Cycle
1 Upregulation
2 Degraded baseline
3 Restoration demand
4 Withdrawal reinforcement
THE DEPENDENCY LOOP — STEP 01
Upregulation
Habitual caffeine use triggers compensatory production of adenosine receptors. The brain adapts to persistent blockade by increasing receptor density.
THE DEPENDENCY LOOP — STEP 02
Degraded Baseline
More receptors means adenosine binds more strongly in caffeine's absence. Baseline alertness falls below the level that existed before habitual use began.
THE DEPENDENCY LOOP — STEP 03
Restoration Demand
Caffeine is now required to return to the previous baseline — not to elevate above it. The substance that degraded the baseline is now necessary to reach it.
THE DEPENDENCY LOOP — STEP 04
Withdrawal Reinforcement
Skipping caffeine produces symptoms that reinforce use, deepening the loop. The dependency is pharmacologically self-reinforcing at each stage.
This has been characterized in the research literature as withdrawal reversal: the notion that much of the perceived benefit of caffeine in habitual consumers is the resolution of the depressed baseline created by prior use rather than a genuine elevation above a non-habituated baseline (Haskell 2005). The evidence here is genuinely contested, and it would be inaccurate to state this as established fact. What the available literature supports is this: the performance and alertness advantage of habitual high-dose caffeine use, measured against a well-rested non-caffeinated baseline, is meaningfully smaller than the subjective experience of caffeine-dependent users suggests.
This does not mean caffeine has no value for habitual users. Acute ergogenic effects on endurance, reaction time, and power output persist even in tolerant individuals, though at attenuated magnitude. The more accurate framing is not that caffeine stops working entirely, but that a significant portion of what it appears to provide is the recovery of function that the dependency itself degraded. The habitual user consuming three cups of coffee per day is not performing at their natural baseline plus three coffees of benefit. They are performing close to their natural baseline, at a cost of three coffees, plus whatever genuine ergogenic effect survives tolerance development.
The habitual user consuming three cups of coffee per day is not performing at their natural baseline plus three coffees of benefit.
For anyone who trains seriously while managing competing demands on their time, sleep, and recovery, the arithmetic of habitual caffeine use is less favorable than the subjective experience of it suggests. The compounding structure this creates is analogous to what happens in overtraining syndrome: the system adapts to chronic overload in a way that makes the original stimulus necessary just to function, while the actual adaptive ceiling drops.
The alertness caffeine provides is, in large part, the recovery of alertness that caffeine-induced adaptation removed.
Does Caffeine Improve Athletic Performance?

Caffeine does produce measurable acute ergogenic effects, and these are well-documented in the scientific literature. Improvements in endurance performance, time-to-exhaustion, power output, and reaction time have been consistently observed in controlled studies, particularly in low-tolerance or caffeine-naive subjects (Goldstein et al. 2010). The mechanism behind the endurance benefit is primarily adenosine blockade reducing perceived exertion at submaximal intensities: the athlete sustains higher output before fatigue perception reaches the threshold that would otherwise reduce effort. This is a real and meaningful effect. It is also, by the definition established earlier in this article, a masking effect rather than a resolution of the underlying physiological state.
LOW-TOLERANCE USER
Genuine Ergogenic Effect
Adenosine receptors at normal density. Caffeine produces meaningful blockade above baseline. Real improvements in endurance, reaction time, and power output.
HABITUAL USER
Primarily Restores Function
Upregulated receptor density means blockade is less complete. Much of the perceived benefit is recovery of the baseline that habituation itself degraded.
For habitual users, the picture is more complicated. Tolerance attenuates the ergogenic effect, and the magnitude of attenuation depends on the degree of habituation. A habitual user who consumes caffeine daily cannot expect the same performance lift that studies conducted with low-tolerance subjects document. What caffeine more reliably provides for the habitual user is performance under conditions where fatigue is elevated: after poor sleep, during a long and taxing training session, or under conditions of elevated cumulative training load. In these contexts, caffeine is effectively restoring competitive function rather than elevating it above a rested baseline.
The correct question for any habitual user is therefore not whether caffeine improves performance in the abstract, but whether it improves performance relative to the alternative of not consuming caffeine given their current habituation state. For many heavy users, the alternative is a baseline that habituation has already degraded. Caffeine helps, but partly because it is addressing the problem it created. The experience described as no motivation to workout is often this mechanism expressing itself before the morning dose has taken effect.
What caffeine more reliably provides for the habitual user is performance under conditions where fatigue is elevated — effectively restoring competitive function rather than elevating it above a rested baseline.
How Much Caffeine Actually Produces a Performance Effect

The evidence-backed range for ergogenic effect in trained athletes is 3 to 6 mg of caffeine per kilogram of body weight, consumed 30 to 60 minutes before exercise (Goldstein et al. 2010). For a 90-kilogram athlete, this is approximately 270 to 540 mg, a range that spans from a large coffee to a significant pre-workout supplement dose. Doses above 6 mg/kg do not produce additional performance benefit in most studies and are associated with meaningfully increased side effects: elevated heart rate, gastrointestinal distress, anxiety, and disrupted fine motor control.
Performance Benefit vs. Dose
0
3
6
9
12
Dose in mg per kg bodyweight. Source: Goldstein et al. 2010.
For athletes in combat sports, that last point is particularly relevant. The skills that matter in BJJ, boxing, or Muay Thai, including timing, precision, and perception of an opponent's movements, are precisely what high-dose caffeine-induced anxiety and motor disruption work against. The dose ceiling is not arbitrary. The underlying reason is the same central governor mechanism that makes perceived exertion a useful signal: disrupting it past a certain threshold produces noise rather than performance benefit.
For habitual users, the effective dose required to overcome tolerance is typically higher than the evidence-backed performance range. Many regular caffeine consumers find themselves dosing primarily to restore baseline alertness, at quantities that approach or exceed the threshold for side effects, while the genuine ergogenic benefit that dose would produce in a low-tolerance user has been substantially eroded by habituation. The dose arithmetic changes significantly when tolerance is factored in, and the direction of that change is not favorable.
Doses above 6 mg/kg do not produce additional performance benefit in most studies and are associated with meaningfully increased side effects.
Caffeine Half-Life and What It Costs After Training

The five-to-six-hour half-life documented in most adults has practical implications that extend well beyond the training session itself (Grzegorzewski et al. 2022). A 300 mg dose consumed at 6 PM leaves approximately 150 mg pharmacologically active at midnight. At 150 mg, caffeine maintains meaningful adenosine receptor occupancy sufficient to delay sleep onset, reduce total sleep time, and suppress slow-wave sleep, the restorative sleep stage most critical for physical recovery and hormonal regulation. The athlete who trains at 7 PM, doses at 6 PM, and considers themselves recovered by the time they go to bed at 11 PM may be systematically degrading sleep quality in ways that accumulate across weeks and months.
300mg @ 6PM → 150mg @ midnight
RESIDUAL ACTIVE DOSE
2.3–9.9 hrs
INDIVIDUAL HALF-LIFE RANGE
Source: Grzegorzewski et al. 2022 (Frontiers in Pharmacology)
This is a distinct mechanism from the crash described earlier. The crash occurs when caffeine clears. The sleep disruption occurs while caffeine is still pharmacologically active. Both represent costs, but they operate at different points in the timeline and are often conflated or addressed separately when they are in fact related. Caffeine consumed too late disrupts the sleep that would clear the adenosine that caffeine deferred; the next morning's adenosine load is higher, and the demand for caffeine to manage it is correspondingly greater.
The degree to which sleep disruption matters varies with individual half-life, which can range from under three hours to nearly ten hours depending on genetic CYP1A2 variation, age, and concurrent medications. A slow metabolizer consuming caffeine at 4 PM may be experiencing significant receptor occupancy well into the following morning. That range is worth knowing, not as a reason to avoid caffeine, but as a variable that determines whether a given timing pattern is working in your favor or against it. A fuller treatment of how caffeine disrupts sleep architecture, including slow-wave sleep specifically, belongs in the companion piece on how much sleep athletes need.
The crash occurs when caffeine clears. The sleep disruption occurs while caffeine is still pharmacologically active.
Caffeine After a Bad Night: What the Risk Structure Looks Like

Caffeine can partially restore exercise performance after sleep deprivation, and this is a real and documented effect (Goldstein et al. 2010). Studies show that caffeine at standard doses in the 3 to 6 mg/kg range can return performance to near-normal levels after one night of partial sleep loss. For an athlete who occasionally trains after a genuinely poor night (unavoidable, not a pattern), this is a reasonable tool to have available.
ACUTE USE
Reasonable Tradeoff
Single night of poor sleep, caffeine restores near-normal performance. Higher adenosine load means steeper crash, but cost is bounded and one-time.
SYSTEMATIC USE
Compounding Problem
Caffeine disrupts next night's sleep via half-life effects, increasing tomorrow's adenosine load, requiring more caffeine. Each step makes the next step worse.
The cost structure of using caffeine in this scenario is higher than the same dose on a well-rested day. Sleep deprivation increases adenosine load significantly. Caffeine blocks a larger accumulated adenosine signal than it would under rested conditions, which means the rebound when caffeine clears is larger, and the recovery demand imposed on the following night sleep is greater. Caffeine used acutely after a bad night does not eliminate the debt from that night; it defers it further.
The scenario that creates a compounding problem is systematic use: consuming caffeine daily to manage a chronic sleep deficit. The mechanism is identifiable. Caffeine disrupts the quality of the next night sleep via its half-life effects, which increases the adenosine load at the start of the following day, which requires more caffeine to manage, which further disrupts sleep. This is not a metaphor for a vague negative spiral; it is a specific pharmacological loop in which each step makes the next step worse. Distinguishing between acute, occasional use and systematic compensatory use is the practical distinction that matters most for anyone training seriously under sustained adult load. For the same reason, systematic compensatory caffeine use maps directly onto the HPA axis load pattern in overtraining: an adaptation that degrades the system it was meant to protect.
This is not a metaphor for a vague negative spiral; it is a specific pharmacological loop in which each step makes the next step worse.
Caffeine Withdrawal Symptoms: Where the Strategy Breaks Down
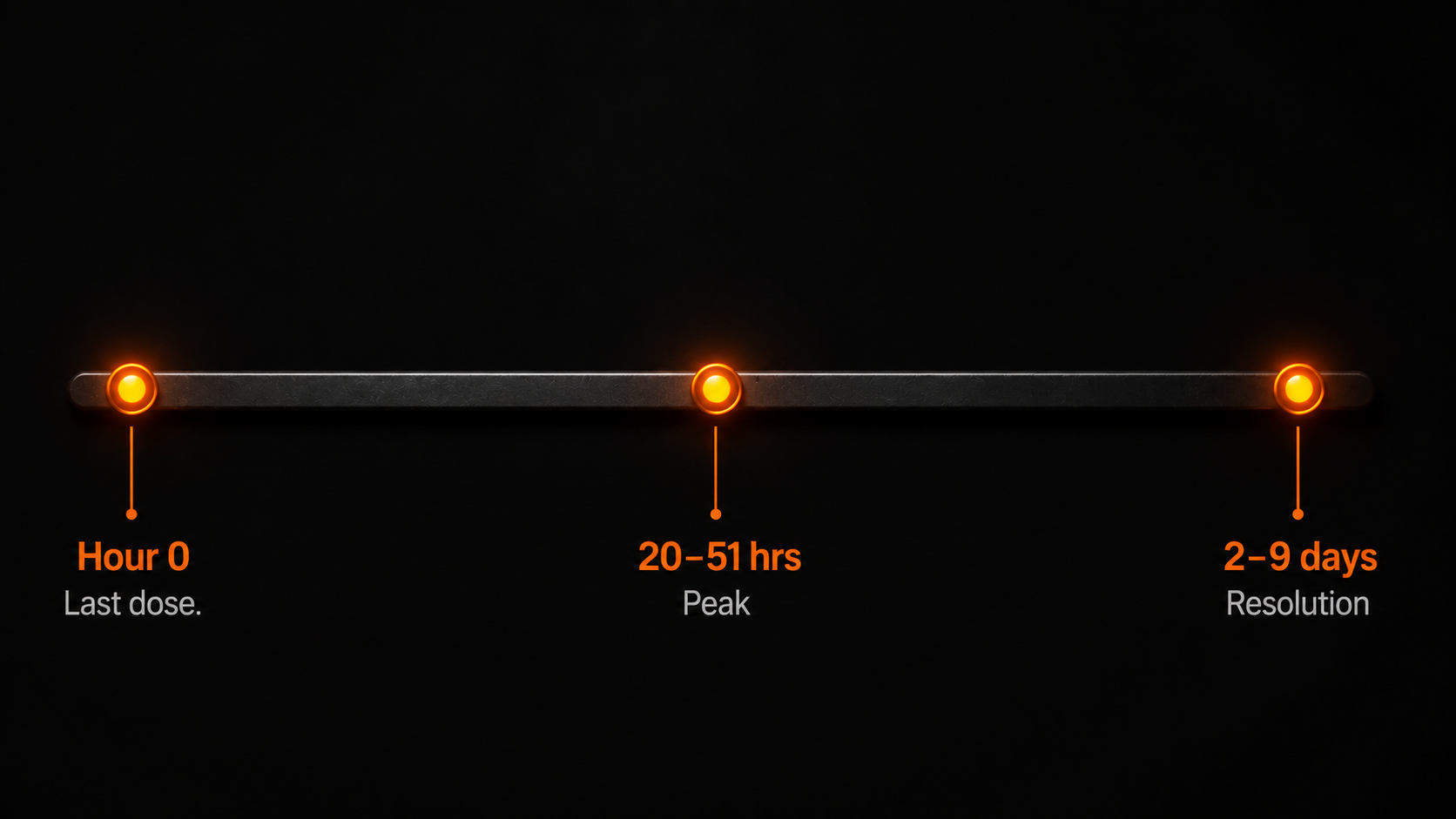
When a habitual user skips their morning coffee and experiences headache, fatigue, difficulty concentrating, and low mood within 12 to 24 hours, the intuitive interpretation is that they need caffeine. The mechanism says something different. Those symptoms, which typically peak between 20 and 51 hours after cessation and resolve within 2 to 9 days in most individuals (Juliano & Griffiths 2004), are evidence of receptor upregulation. The brain has adapted to chronic blockade by producing more adenosine receptors, and those receptors are now fully engaged by adenosine in the absence of the substance that was blocking them.
12–24 hrs
SYMPTOM ONSET
20–51 hrs
PEAK SEVERITY
2–9 days
FULL RESOLUTION
Source: Juliano & Griffiths 2004 (Psychopharmacology)
Withdrawal symptoms are not evidence that caffeine is necessary for normal function. They are evidence that habitual use changed what normal function looks like. A second common error is escalating dose in response to declining effect. Tolerance development naturally reduces perceived impact, and the intuitive response to reduced effect is to increase dose. But higher doses accelerate receptor upregulation, lower baseline alertness further when caffeine is absent, and increase the severity of withdrawal symptoms when the dose is eventually reduced. The loop tightens rather than resolving.
Timing errors produce costs that are easy to overlook because they accumulate at a delay. Given a half-life of five to six hours, a dose consumed at 6 to 7 PM substantially disrupts sleep architecture even when the user falls asleep at their normal time and reports sleeping adequately. The perception of adequate sleep is not the same as adequate slow-wave sleep. An athlete who consistently trains in the evening and doses before training may be experiencing the performance effects of chronically suppressed recovery without connecting that cause to this effect, because the disruption is expressed hours after the dose rather than immediately.
The underlying error across all three of these patterns is treating caffeine as a tool for managing energy when its actual function is managing the perception of energy. That distinction does not make caffeine useless, but it does make a particular set of usage patterns predictably counterproductive.
Withdrawal symptoms are not evidence that caffeine is necessary for normal function. They are evidence that habitual use changed what normal function looks like.
Applying the Mechanism: What Strategic Use Looks Like
The mechanism described in this article does not produce a prescription. It produces a set of constraints that any rational caffeine strategy has to account for. Caffeine is most effective at producing genuine ergogenic benefit when adenosine receptors are not substantially upregulated, when the pre-existing adenosine load is not elevated beyond what the dose can adequately manage, and when the timing does not impose a recovery cost that exceeds the performance benefit. All three conditions favor strategic over habitual use.
Strategic use, in mechanistic terms, means using caffeine at doses and frequencies that produce meaningful receptor blockade without triggering the compensatory upregulation that degrades baseline function. The research on tolerance development suggests that daily use at performance-relevant doses produces upregulation rapidly, and substantially complete tolerance within one to two weeks. Lower doses, less frequent use, or periodic abstention (the latter known in practice as a caffeine washout) are all approaches that the mechanism supports, not as wellness protocols but as rational responses to the pharmacological reality.
HABITUAL USE
Daily Consumption
Produces upregulation, degrades baseline alertness, converts ergogenic benefit to withdrawal management. Tolerance is substantially complete within one to two weeks.
STRATEGIC USE
Scheduled, Periodic
Lower frequency preserves receptor sensitivity. Periodic abstention (caffeine washout) allows receptor downregulation. Ergogenic benefit is maintained across a longer window.
A useful frame is the analogy to training periodization. In the same way that adaptation to training stimulus requires recovery phases that allow the system to absorb and consolidate the stress, caffeine's ergogenic mechanism requires sufficient time without blockade to allow receptor density to normalize. Users who periodically reduce or eliminate caffeine for several days typically report a restoration of baseline alertness and improved caffeine sensitivity on resumption, which is precisely what receptor downregulation following the removal of the upregulation stimulus would predict. The frame is mechanism, not discipline. The reason to periodize caffeine use is not to have willpower about coffee. It is because the pharmacology of the substance rewards strategic use and penalizes habitual use.
The reason to periodize caffeine use is not to have willpower about coffee. It is because the pharmacology of the substance rewards strategic use and penalizes habitual use.
Frequently Asked Questions
Does caffeine actually give you energy, or does it just make you feel less tired?
Caffeine does not generate energy. It is a competitive antagonist at adenosine receptors in the brain, meaning it blocks the signal that accumulates during wakefulness and exertion and progressively reduces alertness. The energy you perceive after consuming caffeine was already present; caffeine suppresses the perception of depletion rather than resolving the underlying metabolic state.
Why do I crash after drinking coffee?
The caffeine crash occurs because adenosine continues to accumulate in the extracellular space throughout the period of caffeine-induced receptor blockade. When caffeine is metabolized and receptor occupancy falls, the accumulated adenosine binds simultaneously. The result is a rapid shift from suppressed fatigue perception to elevated fatigue perception. The crash is not caused by caffeine wearing off; it is caused by deferred adenosine signaling becoming visible all at once.
How long does caffeine withdrawal last?
Caffeine withdrawal symptoms, including headache, fatigue, difficulty concentrating, and low mood, typically begin within 12 to 24 hours of cessation, peak between 20 and 51 hours, and resolve within 2 to 9 days in most individuals. The symptoms reflect adenosine receptor upregulation that developed during habitual use and are not evidence that caffeine is physiologically necessary, but that habitual use altered the receptor landscape.
Does caffeine tolerance mean it stops working?
Tolerance attenuates rather than eliminates caffeine effects. Habitual use produces compensatory upregulation of adenosine receptors, which reduces the degree of blockade a given dose can achieve. Acute ergogenic effects on endurance and performance persist in tolerant individuals but at reduced magnitude. A significant portion of the perceived benefit in habitual users represents recovery of the baseline alertness that habituation itself suppressed.
Is it worth taking a break from caffeine?
From a pharmacological standpoint, periodic abstention allows adenosine receptor density to normalize following the removal of the upregulation stimulus. Users who cycle off caffeine typically report restoration of baseline alertness and improved caffeine sensitivity on resumption. This is a pharmacological consequence of receptor downregulation, not a psychological benefit. The mechanism of caffeine rewards intermittent strategic use and penalizes habitual high-dose consumption. The analogy to training periodization is direct: the system requires recovery phases to restore its adaptive capacity.
The Bottom Line
The central claim of this article is specific: caffeine does not give you energy. It blocks the signal that tells you your energy is depleted. That distinction changes the cost-benefit analysis of relying on it substantially. A substance that generates energy compounds over time as the underlying physiology improves. A substance that masks depletion does not improve the underlying physiology; it defers its signals, creates adaptation that degrades baseline function, and requires ongoing use to maintain a baseline it has itself lowered.
For an athlete who trains under real-world load, including limited sleep, competing demands, and accumulated fatigue from sessions that do not have enough recovery between them, caffeine used strategically has genuine value. It can restore competitive performance under conditions of elevated fatigue, it produces real ergogenic effects when receptor upregulation has not yet attenuated them, and it is available, inexpensive, and reasonably well-characterized pharmacologically. None of this is a reason to avoid it.
What the mechanism does argue against is the specific pattern most habitual users fall into: daily high-dose consumption that produces full tolerance, degrades baseline alertness, disrupts sleep recovery, and converts the primary benefit of the substance from genuine ergogenic effect to chronic withdrawal management. The performance advantage available from caffeine is largest when the system is fresh to it. The dependency loop returns the smallest possible fraction of that advantage at the highest cost.
The performance advantage available from caffeine is largest when the system is fresh to it. The dependency loop returns the smallest possible fraction of that advantage at the highest cost.
If what you want from caffeine is a reliable performance tool, the mechanism argues for treating it like one: used selectively, dosed accurately, timed to avoid imposing recovery costs, and cycled to preserve the receptor sensitivity that makes it work. If you want to understand what a performance strategy without that cost structure looks like, the article on how mitochondria actually work covers the mechanisms that generate actual energy rather than managing its perception.
Caffeine does not produce energy. It delays the perception of a debt that keeps accruing. Every dose without a strategic framework is borrowed time.
The pharmacology of caffeine rewards the user who treats it as a periodic tool. It penalizes the user who treats it as a daily baseline. The mechanism is indifferent to intention.
Mydos Performance
— Sustained vs. Borrowed Energy Series —
Does Caffeine Give You Energy? The Adenosine Mechanism Behind the Crash
The receptor pharmacology of borrowed alertness, tolerance, and the cost your next dose is already paying.
By Ricardo Londono